

Your orthodontist is the medical practitioner who is the best person to evaluate if a combination of orthodontic and orthognatic surgery is necessary.
If a surgical indication is suggested it would be interesting to seek opinions from several medical practitioners.
The main purpose of showing these pictures is to provide you with a better comprehension of our medical techniques.
Each picture outlines aspects of a unique and different clinical situations and could not possibly be transposed.
When to suggest orthognathic surgery ?


Example of a facial disharmony with a backward maxilla and a forward mandible.

This surgical operation restores facial harmony. On the right, the patient has had his jaw advanced, and his mandible pushed backward and an operation on the chin (one single surgery).


The facial harmony was restored by maxillary advancement surgery.
Orthognathic surgery corrects malpositions of the maxilla and the mandible.
The teeth may in some cases be misaligned because the supporting tooth bone structure is mal positioned as a result of lack of growth.
The surgery restores the facial skeleton’s harmony, harmoniously repositioning the upper jaw, and the mandible (with the chin).
The teeth thus find their ideal position.
Prior to the surgery an orthodontic treatment is necessary to align the teeth in accordance with the supporting bone tissue (maxilla and mandibule).
This pre-surgical orthodontic treatment lasts for an average of six to eighteen months.
After the surgery, a short time orthodontic treatment may be necessary.

Dental indication
In case of a significant teeth discrepancy :
The teeth discrepancy is related to jaw malposition.
Orthodontic treatment can not restore the position because the discrepancy is significant.
Surgery is necessary.

If the tooth discrepancy is not significant :
An orthodontic treatment without surgery is possible but in some clinical situations it is preferable to have a surgery.
The surgical indication depends on the axis and the position of the teeth, and your face’s shape (lips volume for exemple), this axis shows the positioning of the maxilla and the mandible.
For example, if the upper lip is thin and the lower teeth are backward, orthodontic treatment without surgery may narrow the upper lip and widen the sulcus between the chin and the lower lip, which could cause premature aging of the face.
A surgery may then be necessary. As a matter of fact, dental mobilization even without surgery causes a facial modification !
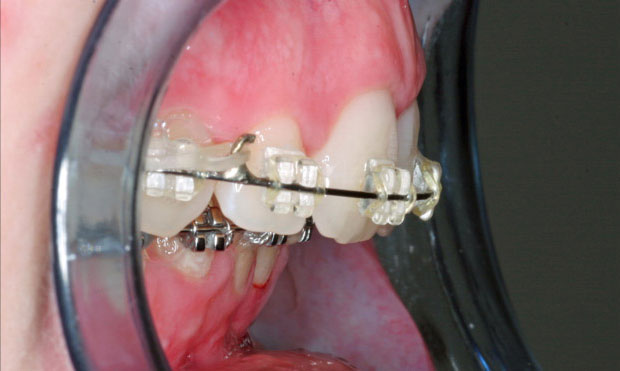
This young girl had a minimal dental discrepancy.
An orthodontic treatment without surgery was possible.
Nevertheless, we had favored an orthodontic-surgical symbiosis to prevent a degra-dation of the facial harmony.
Our patient had a bi-maxillary osteotomy combined with a genioplasty.


Morphological indication

A surgery is necessary depending on the importance of tooth discrepancy and facial disharmony.
Both are the consequences of a growth defect of the mandible that will be surgically corrected.
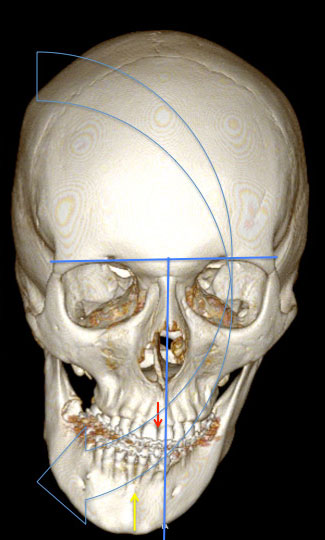
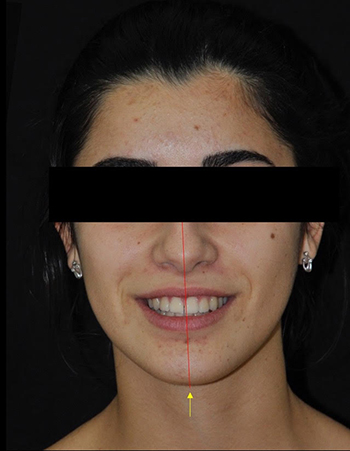
Example of facial asymmetry requiring orthodontic and surgical treatment.
The median axis is shown in blue. The maxilla is deviated to the right (red arrow). The mandible is also deviated to the right (yellow arrow) more significantly.
The face is concave to the right. Surgery will help restoring facial harmony.


On top, an example of a patient showing a gummy smile, adjusted after surgery (shown on the bottom).


Patient suffering from a skeletal Class II ,consequences of a lack of growth of the mandibule.
Postoperative outcome after mandibular advancement surgery and genioplasty.

Correction d’une classe III squelettique et d’une asymétrie faciale par une ostéotomie bi-maxillaire. Résultat après dépose des appareils orthodontiques.
Malposition of the maxilla and mandible is responsible for facial disharmony.
A maxilla too far backward results in a thin upper lip and an wider angle between the nose and the lip.
A maxilla that is excesively high up results in a gummy smile (showing excessive gum when smiling, which is not aesthetic) and lips that don’t touch at rest.
On the contrary an insufficient height of the maxilla results in compressed lips at rest and a toothless smile (we can’t see the teeth, which causes a facial aging).
A mandible too far backward results in a receding chin.
Facial asymmetry may result in a shift of the nasal bone shift, height difference between the left and right sides of the face.
A discrepancy of facial bone structures causes a facial disharmony which is not aesthetic.
A clinical examination associated with analysis of the X-rays and casts will give an accurate diagnosis.
In all cases, a physiological positioning of the bone structures results in a harmonious face.
Functional indication
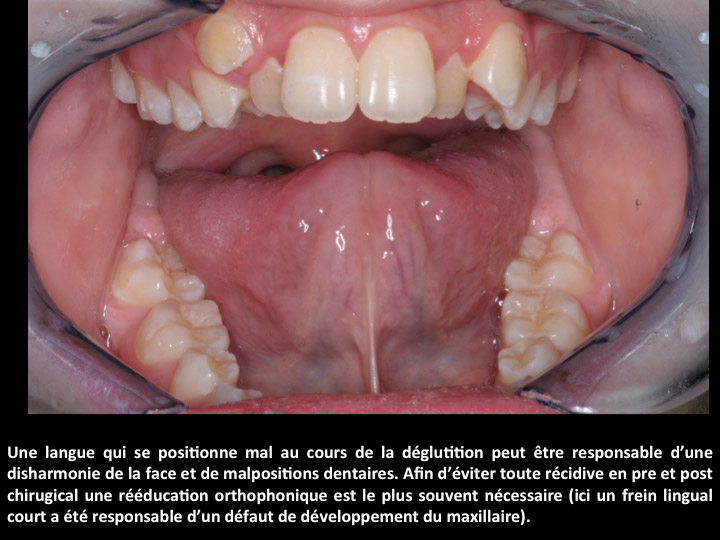
A poor jaw discrepancy treatment may result in periodontal disease (mobility, gingival recession, tooth loss), mouth breathing, poor lingual swallowing position, temporomandibular joint pain, sleep apnea.
Surgery restores facial functions: chewing, swallowing, breathing and allows you to find a satisfactory dental occlusion.
Orthognathic surgery may also be suggested to cure sleep apnea (in some special cases), especially when the mandible is too far backward.


La chirurgie orthognatique permet de corriger l’apnée du sommeil. Nous constatons ici une augmentation du volume des voies aériennes postérieures après une ostéotomie d’avancée bi-maxillaire (au milieu du cercle rouge).
Benefits of orthognathic surgery


Orthognathic surgery restores facial harmony. Our patient has had a mandibular ad-vancement osteotomy associated with genioplasty.


Orthognathic surgery associated with orthodontic treatment has helped restoring a harmonious occlusion (without extraction of premolars) and to preserve facial harmony.
Orthognathic surgery aligns the teeth in an axis that guarantees a better long-term prognosis, restores facial functions (respiratory, masticatory) and facial harmony.
The purpose of this surgery is not to obtain an aesthetic result, but rather to achieve facial harmony, by correcting abnormalities that have occurred during growth.
This harmony is the result of proper physiological function both on the respiratory and dental levels.
The appearance of your face after the surgery is the one you should have had if there had not been any growth disorder.
How is the surgery done ?
Osteotomies are performed orally. There are no visible scars.
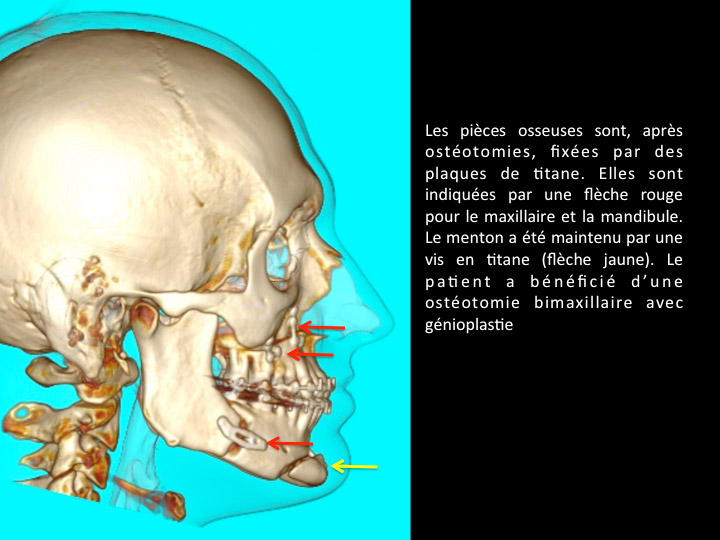
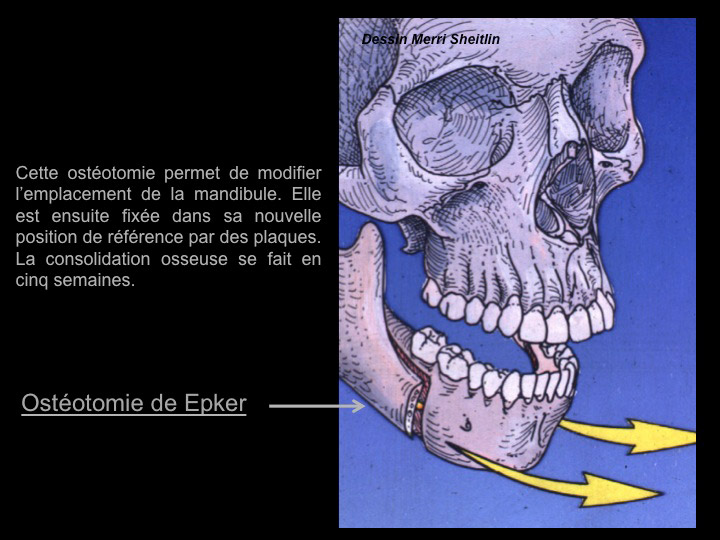
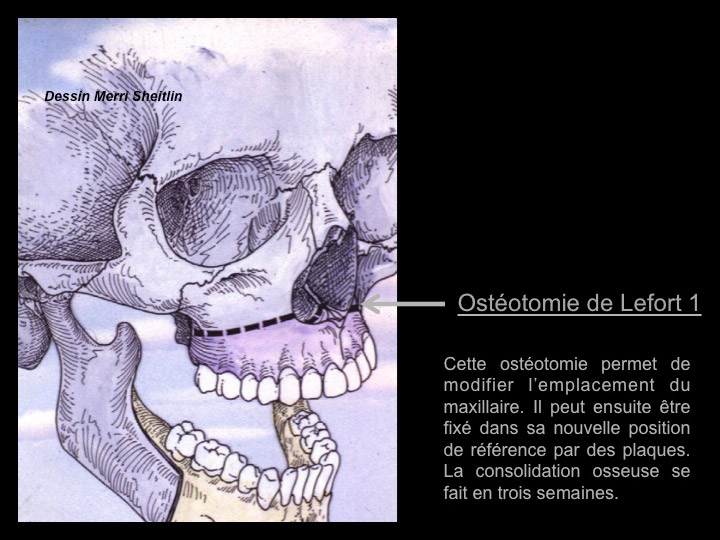
The bone parts are fixed with titanium plates after osteotomy.
The purpose is to allow a quick recovery of the mobility of the jaws.
After bone consolidation, the plates become useless.
However, there is no need to remove them because they are tolerable (except in some cases).
Lefort surgery is an osteotomy of the upper jaw.
Epker surgery is an osteotomy of the lower jaw.
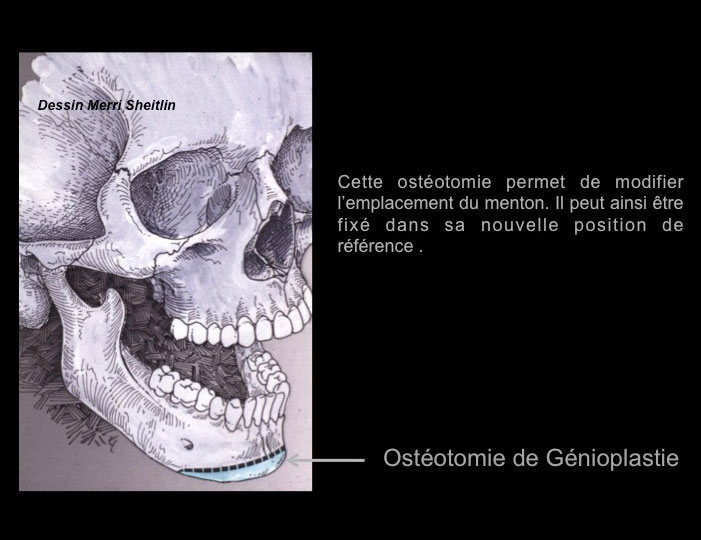
The Genioplasty procedure is a chin osteotomy.
When the osteotomy concerns the upper and lower jaws, it is called a bimaxillary osteotomy.


Patient with a chin too far backward.
Postoperative outcome after genioplasty of advancement.
Genioplasty is an operation with minor post operative adverse effects, you can re-sume your normal activity 5 days after the surgery.
Before the operation

Orthodontic preparation is most often mandatory.
A consultation with the surgeon with a dental panoramic, face and profile X-rays and casts will help the doctor to evaluate different aspects of the case.
The germs of wisdom teeth can in some cases be removed three months before the surgery.
However, in some cases they can be preserved or removed during orthognathic surgery.
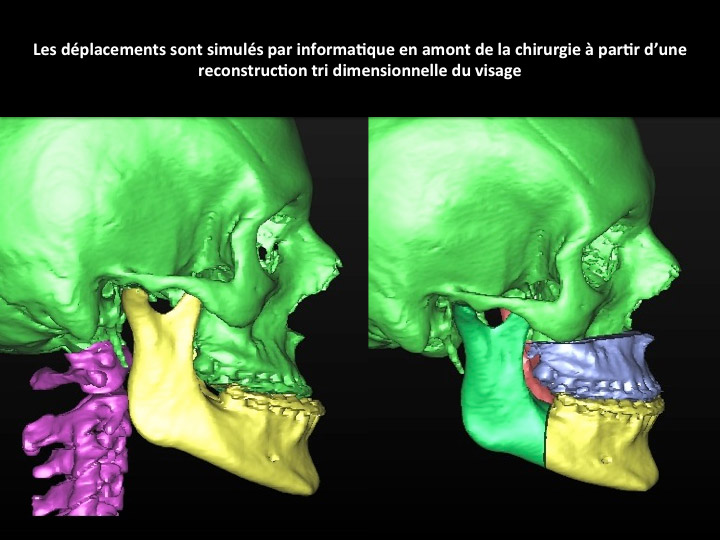
A scanner will be required to secure the osteotomy procedures and to planify displacements with a three-dimensional modeling.
An intermediate dental retainer will be made one month before the surgery.
Its aim is to replace the bone structures in a very precise way and in conformity with the simulations made before the surgery.
The surgeon uses casts to verify the consistency of the inter-arch.
Otherwise the surgery is postponed.
Informed consent, an information sheet and a quote are given to you.
The orthodontist will place the surgical arches and brackets one or two days before the surgery.
These arches and brackets will allow the surgeon to block the jaw during the procedure.
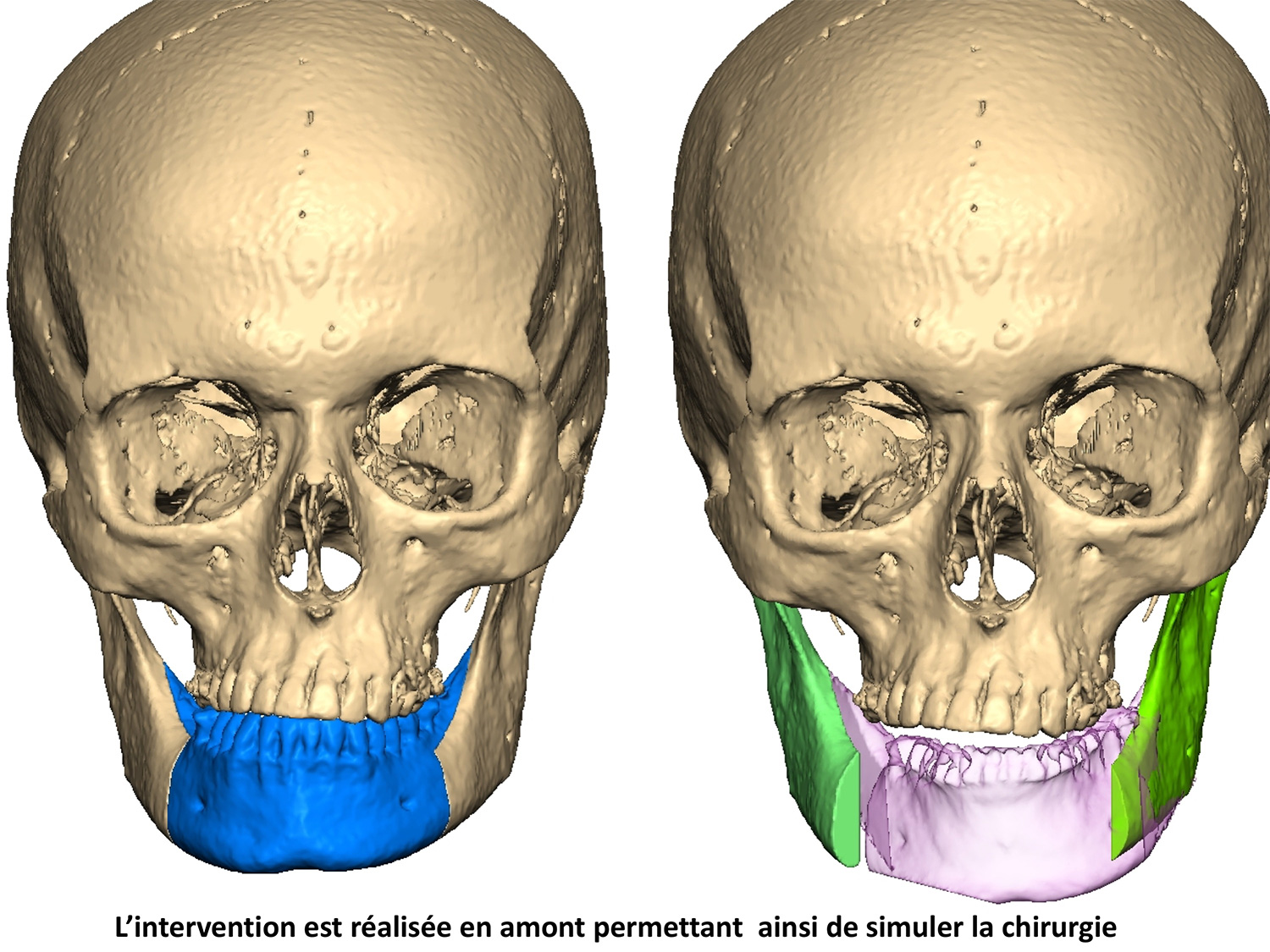
Each surgical intervention is prepared in advance with a three-dimensional analysis and a simulation of displacements.
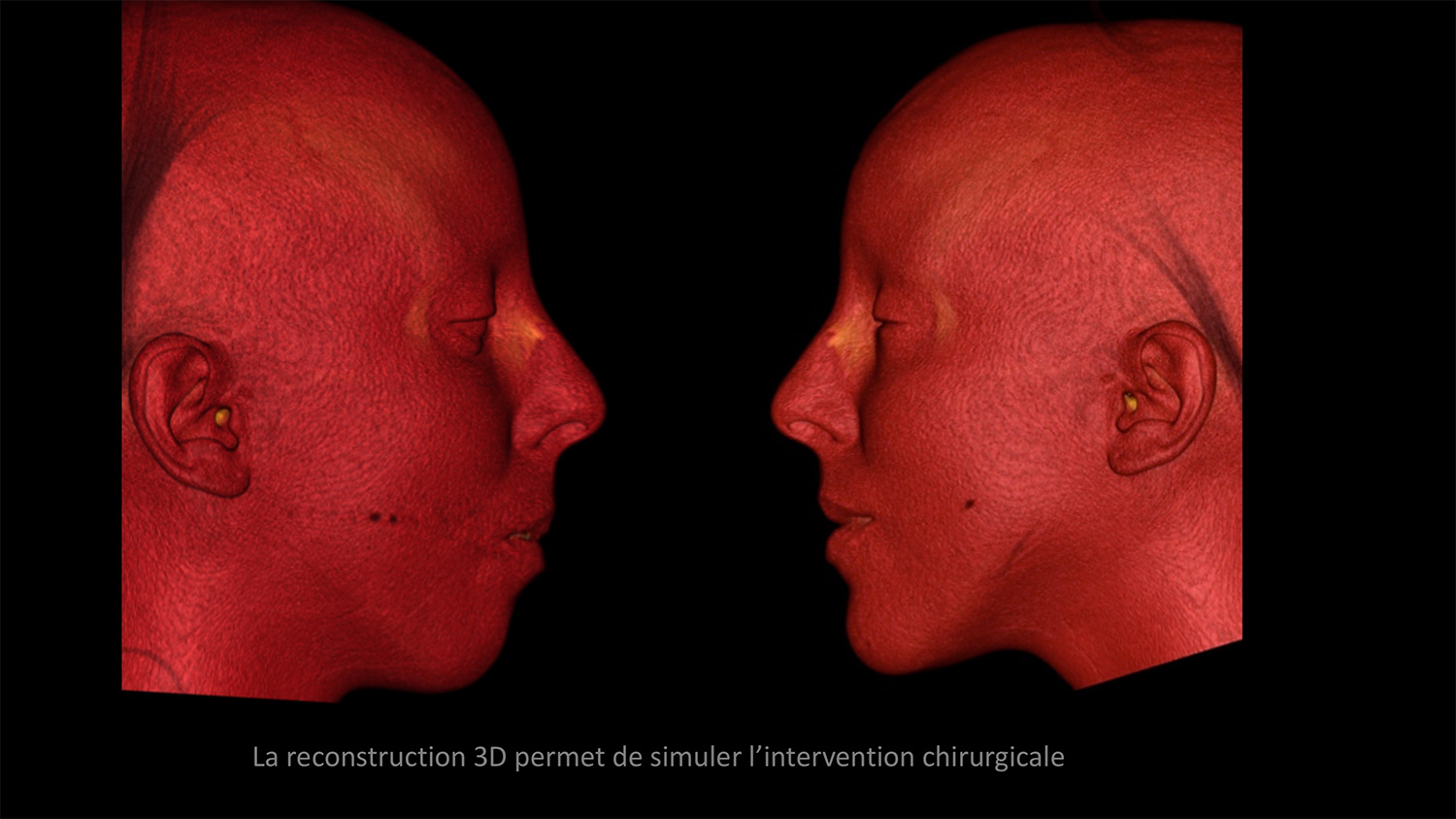
It is more difficult to simulate the consequence of displacements on the soft tissues, as shown here on the 3D scanner.
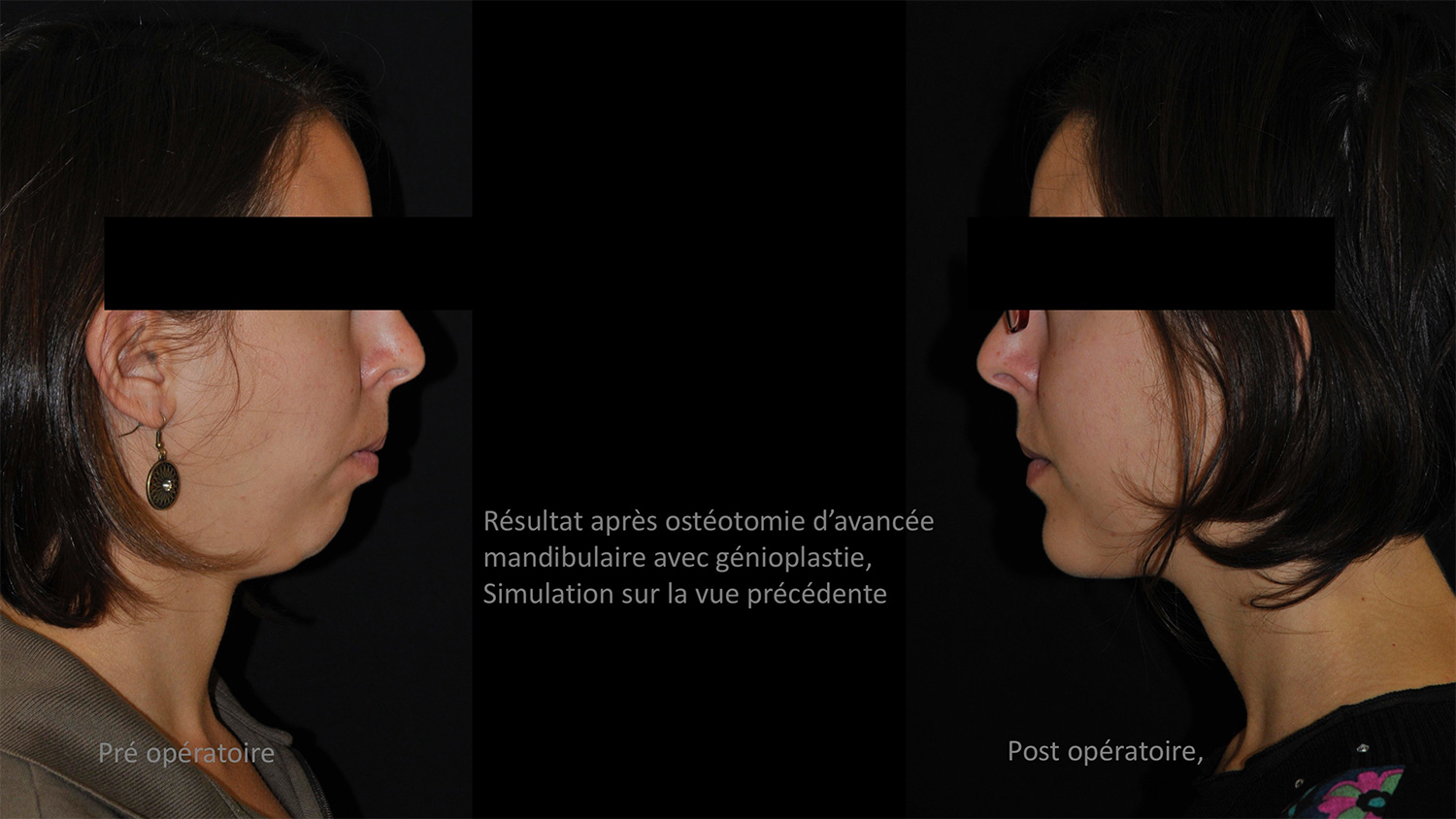
Final result after simulation and surgery.
Hospitalization and after surgery follow-up
You are hospitalized the day before the surgery.
You should bring the last cast and x-rays with you.
The major post operative adverse effects are swelling of the face and sensitivity disorders (as if one had had an anesthesia at the dentist’s).
Short-term hospitalization, 1 to 3 days on average.
Moderate pain can be treated with pain killers.
The swelling of the face is constant. It fades in a fortnight.
Loss of sensitivity of the nose and upper lip occurs in the case of maxillary osteotomy. It will go back to nomal.
The loss of sensitivity of the lower lip occurs in the case of osteotomy of the mandible. In most cases sensibility will completely be restored within few weeks or few months but sometimes a numbness of a part of the lip or chin persists.
Jaw lock is no longer common.
In most cases plates fixing bone structures can avoid the jaw lock.
However, if a jaw lock is necessary, it is not permanent: the elastics can be removed to eat and wash your teeth.
Soft food, not liquid, you can eat almost normally, soft food: mashed potatoes, ground beef, fish, etc …
Dental cleaning should be done with a soft surgical toothbrush and a dental jet.
You should get back to your Orthodontic treatment as early as the third week after the surgery.
Treatment by a physical therapist and maxillofacial orthophonist should start as early as the day after the surgery. This protocol was developed in our service more than ten years ago, it aims for a quick recovery.
After surgery follow-up with the surgeon will continue as long as orthodontic treatment lasts.
You can resume your non violent physical activity as early as the third day after surgery.
You can get back to your personal activities one week after the surgery.
Most often, after fifteen days you can go back to work, however this can change and depends on the postoperative outcomes.


Patient au 10ème jour post-op ici à droite. Notre patient ne présente pas une tuméfaction importante mais dans certains cas elle peut être plus importante.
Complications
Loss of sensitivity of the lower lip and chin :
This is the most frequently described complication.
Unless the nerve is damaged, the sensitivity gradually returns to normal, but a more of less important numbness of the lip and the chin may persist.
Infection :
Very rare complication.
In some cases, a surgical drain is necessary.
Hematoma :
Very rare complication.
With no consequences but may require a surgical drain.
Delay of bone consolidation, “pseudoarthrosis” :
Very rare complication.
Jaw lock may be necessary.
Or an occlusal treatment.
Or a surgical revision with bone grafts.
Other complications have been described but with an extremely rare probability.
Some internet links, some movies which can help you :
- A site that explains orthognathic surgery : http://myoms.org/procedures/corrective-jaw-surgery
- A video to understand orthognathic surgery : https://youtu.be/JP-8mqLcYbs
- A testimony : https://youtu.be/fq84Lsa9Ni8

